The tragedy that unfolded in Canada’s nursing homes trained a wider public lens on the demographic and economic challenges facing the country’s patchwork eldercare model.
These problems, decades in the making, were already in need of attention given Canada’s aging population. COVID-19 highlighted the urgency of addressing existing challenges while raising new questions around eldercare. They include how best to prevent the transmission of infection by underpaid support workers moving between multiple homes, and how to better protect vulnerable residents.
As painful as the crisis in long-term care homes has been, it has highlighted the need to modernize an eldercare system built for the Canada of 50 years ago, not the Canada of the 2020s. It has also created a clear opportunity for Canada to make better use of innovative technologies and funding models to ensure that the growing ranks of older Canadians have access to the best long-term care options available.
Key points
- Out of 14 countries, Canada has the highest proportion of deaths in long-term care (LTC) from COVID-19;
- Even before COVID, LTC costs were expected to more than triple over 30 years, to more than $70 billion in 2050;
- Canada committed 1.3% of GDP to publicly funded LTC services in 2017, compared to an OECD average of 1.7%;
- 35% of Canadians balance paid work with unpaid caregiving, providing an additional $25 billion in care but leaving many at risk of injury and burnout;
- 89% of respondents to a national survey wanted to see more home and community care;
- Canada must spend more, hire more and take a nationwide approach to confronting urgent LTC issues.
Key questions
1. What has COVID-19 revealed about Canada’s LTC system?
COVID-19 exposed a range of longstanding weaknesses in LTC. Topping the list: insufficient staffing, low wage levels and precarious employment that force many workers to move between jobs in multiple homes—increasing the likelihood of transmission and the risk of infection to themselves and residents.
Canada’s system is supported by hundreds of thousands of healthcare professionals, but it is the largest group—unregulated healthcare aides or personal support workers—who are most likely to find themselves in this position.
In Ontario, PSWs who work in LTC earn between $14 and $16 an hour, less than two-thirds of what their counterparts earn in hospitals. As a result, they often juggle several part-time jobs or exit for better opportunities elsewhere. They report high rates of burnout and dissatisfaction in their positions and frequently cite concerns about unsafe work environments. These conditions have made it difficult to attract and retain people to these roles and by extension, to meet accepted standards of care, including a recommended minimum of four hours of direct care per resident each day, a threshold no Canadian jurisdiction is currently meeting. Roughly 80% of nursing home operators in Ontario reported difficulty filling shifts.
Canada’s LTC system is housed in buildings that were not designed for the current challenges confronting the elderly population. Many of these homes were designed in the 1960s and feature multi-bed wards which have been found to accelerate the spread of infection. Indeed, the operations hardest hit by COVID were those in homes with multi-bed rooms.
The results are stark: One in 50 LTC residents in Ontario has died of COVID, far eclipsing the number of deaths among older Ontarians receiving home care.
Minimum staffing levels, improved wage rates and the elimination of sectoral pay gaps would help draw more people to critical PSW roles, enabling the development of surge capacity that would ensure a larger, prepared labour force in times of crisis. A concerted push to retrofit existing LTC homes to modern standards would help improve care and safety.
2. How well was Canada’s eldercare system performing before COVID?
Canada’s LTC system was already struggling to meet the needs of a population that is living longer and experiencing more complex problems. Canada’s universal health system was built in the 1960s, when the average age of Canadians was 27 and life expectancy was less than 70 years. Today, the median age is 40.8 years and life expectancy is over 80. By 2030, nearly one in four Canadians will be older than 65.
What’s more, the system is unbalanced: more than 40,000 Canadians are on wait lists for nursing homes due in part to a lack of home and community-based care. A further 20,000 are in ALC (alternate level of care) designated beds, that is, occupying more costly hospital beds due to a lack of available LTC spots. The problem is especially acute in Nova Scotia, where one-third of all hospital beds are occupied by ALC patients.
The problem will only get worse. About 650,000 people will be living in seniors’ residences or nursing homes in 2030, up from 450,000 now. Public and private resources needed to build the extra capacity will be at least $140 billion.
Crucially, the system itself, which devotes the majority of resources to LTC homes, is ill-fitted to provide the type of care that various surveys have suggested Canadians actually want. A 2015 survey by Ipsos Public Affairs found the majority preferred care in or close to home. And the Canadian Institutes for Health Information found that 22% of Canadians who were entering nursing home environments may have been able to receive care at home with appropriate home care and community-based supports.
3. What’s the long run fiscal impact of shifting to a system focused on home and community-based care?
That’s hard to say, though various research institutes are looking into what this could mean for Canada.
The country was already spending less than other industrialized countries on LTC, committing 1.3% of GDP to publicly funded long term care health services in 2017, compared to an OECD average of 1.7%. And even before COVID, costs for LTC were expected to more than triple over 30 years, from $22 billion today to more than $71 billion in 2050.
In long-term care spending, Canada is in the middle of the pack
Share of GDP (2017 or latest year), %
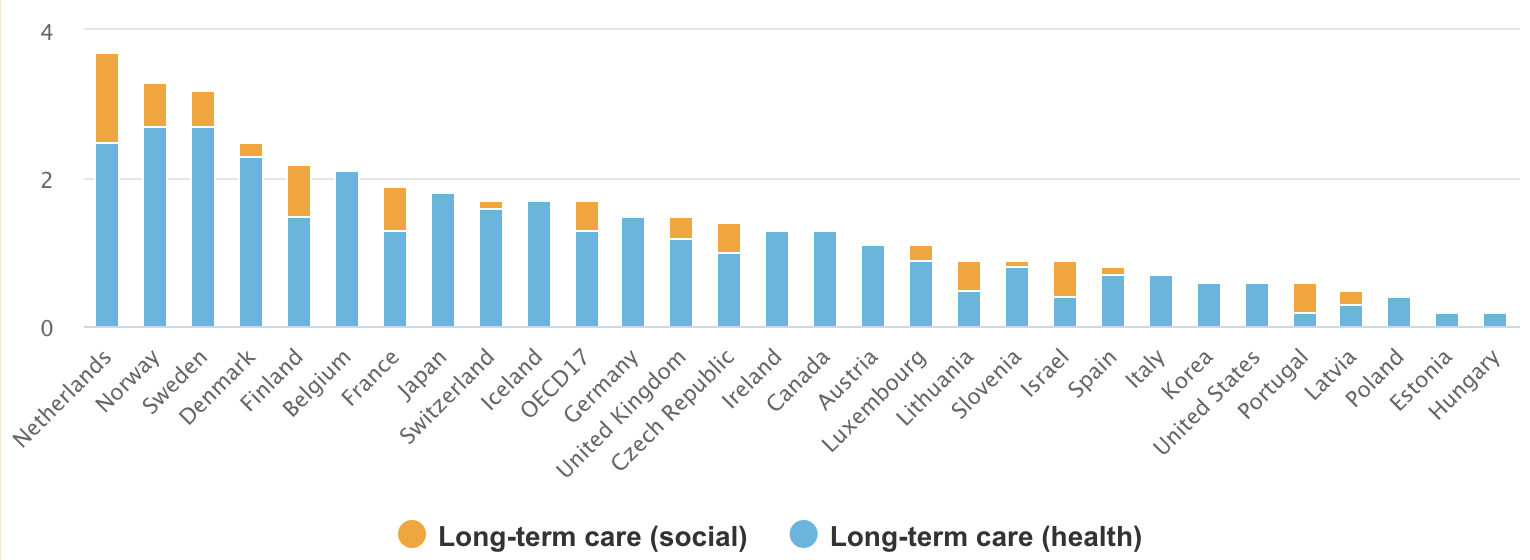
Source: OECD, RBC Economics | * OECD17: average of 17 OECD members reporting both health and social long-term care spending
It’s clear Canada will have to spend more. But home-based care has the potential to be more cost efficient. The average per diem cost of a hospital bed in Ontario for instance, is $842, compared to $126 for LTC and $42 for home care. Similar gaps exist across the country.
Focusing on home and community-based care will mean making a major shift in the way funding is allocated. About $6 billion of a total $33 billion in public and private LTC funds was spent on home and community-based care in 2018.
And shifting to home-based care could entail significant upfront costs. Canada will have to spend more on everything from recruiting more PSWs and improving their pay to providing better support for the nearly 8 million Canadians (often family members and neighbours) who provide unpaid care to aging people in their homes.
International examples suggest the cost curve bends down over the longer term. Thirty years ago, Denmark faced similar demographic pressures to Canada. It chose to focus future healthcare spending in the home and community care sector. Today, 36% of Denmark’s LTC funding is spent on designated buildings or nursing homes and 64% on home and community care—a reversal of the OECD average that saw 65% of funding spent on nursing homes and the remainder on home and community care.
This shift enabled Denmark to avoid building any new nursing homes for close to 20 years and to close thousands of costly hospital beds. It saw a 12% reduction in overall LTC expenditures on the population aged 80 or older in the first decade of its approach.
At 2.5% of GDP, Denmark spent more on LTC between 2005 and 2015 than the OECD average of 1.7%. But its spending growth rate – also 2.5 per cent – is well below the OECD average of 4.6%. Canada’s spending growth rate over the same period was 2%.
4. What role can technology play in allowing more Canadians to age at home?
Emerging technologies can play a critical role in providing better, more cost-efficient outcomes for patients, and reducing or delaying hospital and LTC admissions.
Beyond exposing some of the vulnerabilities in Canada’s eldercare system, COVID 19 has revealed a number of opportunities in this arena. Indeed, the lockdown restrictions have shown that virtual visits with doctors and other care providers can work well and reduce the need for transportation to appointments. Other examples of technologies that allow for assisted living and greater independence are scattered throughout the country and the world.
In Ontario, the Canada Health Infoway’s Community Paramedicine Remote Patient monitoring project has reduced 911 calls and hospital admissions and generated more than $7,000 per patient annually in cost savings. Under the program, paramedics provide patients with Bluetooth-enabled devices like weight scales, blood pressure or heart rate monitors and a transmitting device that sends their biometric data to local community paramedics to allow for real time monitoring.
Other examples include ambient living sensors to monitor adults at risk of falls in their homes and to collect data that can assist in the development of future innovations.
Beyond devices, new community-based models of living outside nursing homes are emerging, including multifamily homes where younger members care for older family members, and co-owned homes and shared living among unrelated elderly Canadians.
5. What else is required?
Enabling more Canadians to age in their homes will have to include supports for family and community carers, including training, counselling services and some financial support. The majority of the 8.1 million Canadians providing care to chronically ill, aging or disabled family members or friends lack adequate support. More than 6 million Canadians are balancing these duties with paid work. And many are making this contribution despite having low incomes themselves. Grants and tax relief programs, including refundable tax credits, have been implemented effectively in Quebec, Manitoba and Nova Scotia among other provinces.
Failing to address the needs of unpaid carers, along with those of paid healthcare professionals could lead to burnout and has been identified as a threat to future economic productivity.
Enduring issues in the structure, funding and public understanding of Canada’s eldercare model also exist. In many ways these issues are interrelated. Indeed, the Canada Health Act, created in 1984, focuses on hospital and physician services but does not address the universal LTC. With no established federal standards, or even a single definition across all provinces of what services it consists of, a patchwork of provincial delivery models (including different variations of public and private services), eligibility and spending has emerged, together with a system of inconsistent, insufficient data collection to measure outcomes.
This makes it difficult for Canadians to understand or plan for their own care.
6. What’s next?
To chart a course to a better system in the wake of COVID-19, Canada’s LTC system must confront both new challenges related to infection control and longstanding concerns about the system itself. The most urgent concerns are also those that will contribute to a better model: retrofitting aging homes to include single-bed wards and improving pay wages and availability of full-time positions for PSWs.
Shifting the system to provide the kind of eldercare Canadians desire is also essential, as is increasing public funding—although this likely won’t be enough to cover the entire cost. Bold decisions need to be made together with Canadians about how private, not-for-profit and public sectors will be involved.
As it stands, 63% of Canadians say they aren’t in a good position financially or other wise to pay for their care. And due to differing systems and definitions, many are uncertain of what that will entail. Greater clarity on the system and what care they will need to pay is critical.
This article is intended as general information only and is not to be relied upon as constituting legal, financial or other professional advice. A professional advisor should be consulted regarding your specific situation. Information presented is believed to be factual and up-to-date but we do not guarantee its accuracy and it should not be regarded as a complete analysis of the subjects discussed. All expressions of opinion reflect the judgment of the authors as of the date of publication and are subject to change. No endorsement of any third parties or their advice, opinions, information, products or services is expressly given or implied by Royal Bank of Canada or any of its affiliates.